What is Frozen Shoulder?
Frozen shoulder is a common cause of shoulder pain in the adult population. Symptoms consist of pain and stiffness of the shoulder. Patients often notice a sudden onset of pain when reaching backwards. The cause is often unknown but is common in diabetics and women in their 40’s and 50’s. Treatment is geared toward physical therapy to improve range of motion and pain control with cortisone injection and NSAID’s. Arthroscopic surgery to improve range of motion is reserved for those who fail non-operative treatment.
Capsular Release for Frozen Shoulder
Pathology and Treatment:
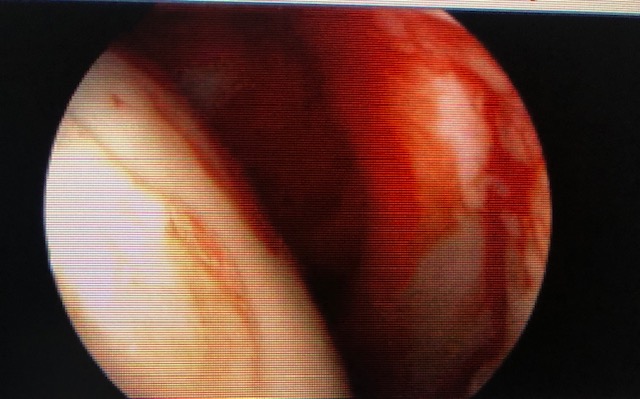
The underlying pathology in an idiopathic frozen shoulder is abundant glenohumeral synovitis, which results in pain and capsular thickening with subsequent loss of motion. Patients will first lose internal rotation (rotation behind the back) and then forward elevation (elevation overhead) and finally external rotation with the arm at the side (rotation outward). It is frequently diagnosed as impingement initially but is secondary to the tight posterior capsule. The tightness causes anterior/superior translation and subsequent impingement (subacromial) with forward evaluation. This particular diagnosis is noted mostly in diabetics and females.
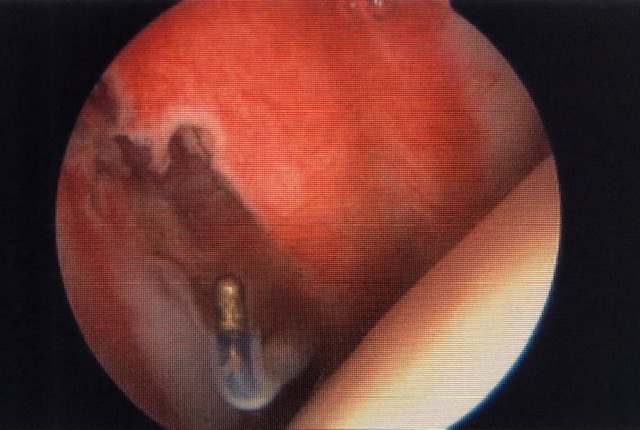
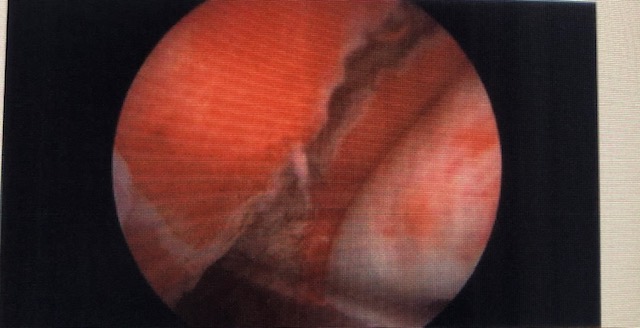
Initially, adhesive capsulitis is treated with an intra-articular steroid injection and subsequent stretching focusing on long slow stretches. The stretching should be started within 4-5 days after injection. If this non-operative treatment fails, then arthroscopic extensive debridement capsular release is performed. Stretching will begin immediately to maintain range of motion gained in the operating room. Sling will be discontinued immediately after the block wears off.